Pain, discomfort or sleep loss from bouts of heartburn?
- At July 13, 2017
- By Site Administrator
- In News
 0
0
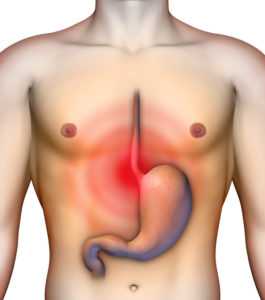 The word heartburn may well describe the sensation of acid reflux, but it fails to communicate the part of the body where damage can occur: the esophagus.
The word heartburn may well describe the sensation of acid reflux, but it fails to communicate the part of the body where damage can occur: the esophagus.
Sometimes called the food pipe, the esophagus delivers everything we eat or drink to the stomach. The esophagus keeps food there by way of a muscular valve that prevents the backflow of digestive juices; the body’s normal and specialized combination of hydrochloric acid, potassium chloride and sodium chloride.
The actual term for chronic heartburn is gastroesophageal reflux disease, or GERD, a condition where acid from the stomach flows backwards into the esophagus and over time can lead to serious complications; one being a pre-cancerous condition called Barrett’s Esophagus.
But how does one know if they have GERD versus a little tummy trouble? Check the following list and see if you have symptoms.
You might experience…
- A burning sensation that moves up and burns the back of your throat
- An acid taste in the mouth
- Reflux after meals and during the night
- Reflux more than twice a week
- Only temporary relief from over-the-counter antacids
Some people may also have a chronic cough or wheezing. These seemingly unrelated symptoms could also indicate GERD.
So if you’re having two or more of any of these symptoms, talk to your doctor. There are lifestyle changes your doctor will recommend, such as losing weight and avoiding trigger foods. However, if lifestyle changes don’t help, you might have a weakened ‘valve’ and this is a physical issue that requires treatment to help protect the esophagus.
There are different classes of medications your doctor can prescribe, and sometimes you may have to switch medications if symptoms return. The doctor may also order diagnostic tests such as endoscopy or an upper GI series.
Written by: MaryAnne Pankhurst
Rheumatoid Arthritis: Shifting the focus from control to cure
- At May 25, 2017
- By Site Administrator
- In News
- 0
 A decades-long shift in understanding the B-cell arm of the immune system has produced treatments that relieve the joint-destroying inflammation caused by rheumatoid arthritis. However, a group of researchers at New York University Langone Medical Center and the University of Pittsburgh say relapse remains inevitable until research puts underlying defective B cells on centre stage.
A decades-long shift in understanding the B-cell arm of the immune system has produced treatments that relieve the joint-destroying inflammation caused by rheumatoid arthritis. However, a group of researchers at New York University Langone Medical Center and the University of Pittsburgh say relapse remains inevitable until research puts underlying defective B cells on centre stage.
In the study recently published in Arthritis & Rheumatology, Gregg Silverman, MD and colleagues describe their newly designed test for measuring underlying autoimmunity. They recommend that clinical trials for new drug development incorporate the test to shift focus from controlling inflammation to finding a cure for rheumatoid arthritis (RA).
Unlike osteoarthritis, which results from joint wear and tear, RA is an autoimmune disease that destroys and deforms joints, and can also damage the skin, eyes, lungs, heart and blood vessels. The main treatments for RA include methotrexate and TNF inhibitors that control inflammation.
With a focus on defective “memory” B cells that secrete anti-citrullinated protein antibodies, or ACPAs present in the blood of the vast majority of RA sufferers at diagnosis, the study had three main components.
- Assays were used to detect and identify a range of antibodies produced by B cells in cell cultures.
- Blood samples were taken from RA sufferers and non-sufferers, showing high levels of ACPA secreting memory B cells in the blood of people with the autoantibodies, but not in people without autoantibodies or in the people without RA.
- RA sufferers in remission after treatment with either methotrexate or TNF inhibitors were assessed for serum APCA levels with the conclusion that neither treatment is capable of affecting the underlying autoimmunity that causes a relapse.
Written by: MaryAnne Pankhurst
Disease-associated anti-citrullinated protein memory B cells in rheumatoid arthritis persist in clinical remission
Adam J. Pelzek MS1, Caroline Grönwall PhD1, Pamela Rosenthal MD1, Jeffrey D. Greenberg MD1, Mandy McGeachy PhD2, Larry Moreland MD2, William F.C. Rigby, MD3, and Gregg J. Silverman MD1.
Being Under or Overweight Can Increase Risk for Migraines
- At May 15, 2017
- By Site Administrator
- In News
- 0

While science has advanced the understanding, treatment, and prevention of migraines far beyond that of the pre-scientific era, many avenues of research remain. However, a new study has shown that being either under or overweight can increase a person’s risk for developing the painful, often debilitating condition that has plagued humankind since it was first described in Babylonian documents 5,000 years ago.
Published in the journal Neurology in May 2017, a meta-analysis conducted by Bezu Gelaye and colleagues pooled data from 12 studies involving close to 290,000 research participants. Results demonstrated a 13 percent increase in risk for those with a BMI under 18.5 and a 27 percent increase in risk for those with a BMI over 30.
For context, researchers conducting the meta-analysis considered the link between body weight and migraine risk to be moderate and similar to the link between migraines and ischemic heart disease and/or a migraine and bipolar disorder.
The meta-analysis also showed that obesity and the occurrence of migraines are more common among women and in younger people. But the authors say more research would be necessary to determine why, and whether helping people to establish and maintain a healthy weight would lower the risk for developing migraines.
It is presently estimated that migraines affect more than 700 million people worldwide, and that attacks can last anywhere from 4 to 72 hours. In addition to pain, migraines also cause nausea, vomiting, photophobia and phonophobia – the latter being an aversion to sound that can extend to the sound of one’s own voice.
Written by: MaryAnne Pankhurst
http://www.neurology.org/content/early/2017/04/12/WNL.0000000000003919.abstract
Bizu Gelaye, PhD, Simona Sacco, MD, Wendy J. Brown, PhD, Haley L. Nitchie, BS,
Raffaele Ornello, MD and B. Lee Peterlin, DO
Bone Mineral Density (BMD) calculator
- At May 03, 2017
- By Site Administrator
- In News
- 0
 The Bone Mineral Density (BMD) calculator was created as a tool to help you take initiative in your own health and educate yourself on whether or not you need a BMD scan. The formulated questions, along with your subsequent responses, will generate an answer as to whether or not you should consider booking a BMD appointment. Please answer all questions honestly for an accurate response. If you have further questions following your results, feel free to discuss them with the doctor during your next appointment. Get started now by clicking below!
The Bone Mineral Density (BMD) calculator was created as a tool to help you take initiative in your own health and educate yourself on whether or not you need a BMD scan. The formulated questions, along with your subsequent responses, will generate an answer as to whether or not you should consider booking a BMD appointment. Please answer all questions honestly for an accurate response. If you have further questions following your results, feel free to discuss them with the doctor during your next appointment. Get started now by clicking below!
BMD Calculator
Online Cognitive Behavioral Therapy for Chronic Pain and Mental Illness
 Chronic pain is extremely debilitating, both physically and mentally. When physical pain is a problem in your life, more often than not, you begin to develop stress about the situation, leading to more pain and a severe impact on your mental well-being – it is a vicious cycle. People in these situations often turn to substances or distractions to cope with the present situation. There is a dire need for an easily accessible program that provides mental health support to chronic pain sufferers all over the world.
Chronic pain is extremely debilitating, both physically and mentally. When physical pain is a problem in your life, more often than not, you begin to develop stress about the situation, leading to more pain and a severe impact on your mental well-being – it is a vicious cycle. People in these situations often turn to substances or distractions to cope with the present situation. There is a dire need for an easily accessible program that provides mental health support to chronic pain sufferers all over the world.
The Wilderman Medical Clinic Internet Cognitive Behavioral Therapy (iCBT) program consists of 8 modules of online cognitive behavioral therapy and mindfulness. This program targets individuals of all ages suffering from chronic pain and co-morbid anxiety and/or depression. Anyone suffering from a chronic debilitation (such as stress or injury) will be able to benefit.
Each of the 8 modules follows a sequential order that builds upon concepts in previous modules. They consist of information to read and comprehend at your own pace, interactive activities, and end-of-module homework.
Various research studies have shown the efficacy of iCBT. A review on various iCBT programs revealed that in 7 trials, between 43% and 86% of chronic pain patients had significant decreases in pain intensity1. Results of this review demonstrated that online CBT is effective for individuals with fibromyalgia, back and neck pain, and mixed etiology chronic pain1. A study conducted on a physician-directed 5-module iCBT program for pain showed positive results. The treatment group achieved significantly greater improvements than controls in levels of anxiety, depression, and average pain levels after completion of the program2.
Written By: Rachel Berkovich, HBSc
References:
1. Knoerl, R., Lavoie Smith, E., & Weisberg, J. (2016). Chronic Pain and Cognitive Behavioral Therapy: An Integrative Review. Western Journal of Nursing Research, 38(5), 596-628. doi:10.1177/0193945915615869
2. Dear, B. F., Titov, N., Perry, K. N., Johnston, L., Wootton, B. M., Terides, M. D., . . . Hudson, J. L. (2013). The Pain Course: A randomised controlled trial of a clinician-guided Internet-delivered cognitive behaviour therapy program for managing chronic pain and emotional well-being. Pain, 154(6), 942-950. doi:10.1016/j.pain.2013.03.005